I’m pleased to share that my paper, “The Trigeminal Triad: A Rate-Dependent Model Linking Neurovascular Compression, Vascular Pulsatility, and Sleep-Disordered Breathing in Trigeminal Neuralgia,” has been accepted for publication in Medical Hypotheses, an Elsevier journal.
As an acupuncturist and practitioner of Classical Chinese Medicine, one of the most ancient holistic medical systems in the world, I was trained to look for patterns and relationships across the whole person rather than viewing symptoms in isolation. We call this approach “treating the root and the branches.” In clinical practice, this means paying attention not only to the site of pain, but also to sleep, circulation, stress physiology, inflammation, digestion, breathing, emotional strain, and the body’s capacity to repair.
Over the last decade, while treating and observing patients with trigeminal neuralgia, I noticed a recurring pattern: several patients also had signs of vascular dysregulation, pulsatility-related issues, significant sleep disturbance, or diagnosed or suspected sleep-disordered breathing. These observations did not prove causation, but they raised an important question:
Could trigeminal neuralgia sometimes emerge from an interaction between nerve vulnerability, vascular stress, and impaired repair capacity?
That question eventually led me to develop the Trigeminal Triad hypothesis and write this paper.
The accepted explanation for many cases of classical trigeminal neuralgia is neurovascular compression (NVC) — a blood vessel pressing on or irritating the trigeminal nerve near the brainstem. This remains an important and well-established cause.
But there is also a conundrum: studies have found that vascular contact near the trigeminal nerve can appear in people who never develop trigeminal neuralgia, while some patients with trigeminal neuralgia do not show clear compression. In other words, anatomy matters, but anatomy alone may not explain why the condition becomes symptomatic in some people and not others.
The Trigeminal Triad hypothesis builds on the neurovascular compression model rather than replacing it. It proposes that trigeminal neuralgia may be better understood as a possible injury–repair imbalance involving structural vulnerability, vascular pulsatility, and systemic factors such as sleep-disordered breathing or chronic intermittent hypoxia.
Without medical jargon, the Trigeminal Triad hypothesis asks:
What if trigeminal neuralgia emerges when stress on the trigeminal nerve exceeds the body’s ability to repair and stabilize that nerve over time?
Why this hypothesis matters
Trigeminal neuralgia is often described as one of the most severe pain conditions known. It can cause sudden, electric-shock-like facial pain triggered by ordinary activities such as talking, chewing, brushing the teeth, shaving, touching the face, or exposure to wind.
The most established explanation for classical trigeminal neuralgia is neurovascular compression (NVC), where a blood vessel contacts or compresses the trigeminal nerve near the brainstem.
But many people have blood vessel contact near the trigeminal nerve and never develop trigeminal neuralgia. Also some people develop trigeminal neuralgia without clear evidence of compression. And some people improve after treatment but later experience recurrence.
The Trigeminal Triad hypothesis was developed to help think through those clinical realities.
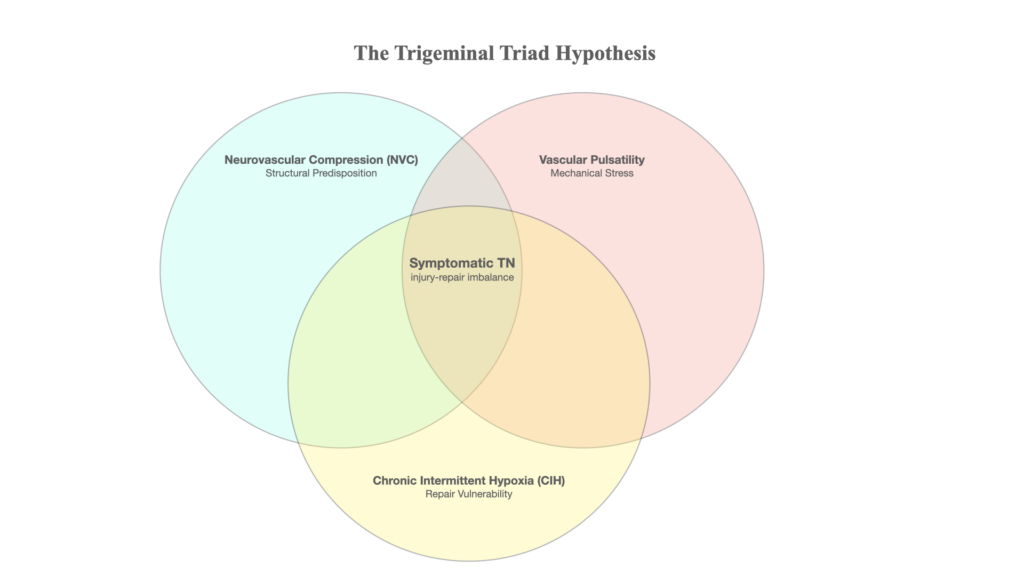
It proposes that trigeminal neuralgia may emerge from the interaction of three possible domains, though it could also occur by any of these three:
- Neurovascular compression
A structural vulnerability near the trigeminal nerve root. - Vascular pulsatility
Mechanical stress from pulse pressure, arterial stiffness, or abnormal vascular movement. - Chronic intermittent hypoxia
Repeated drops in oxygenation, often associated with sleep-disordered breathing such as obstructive sleep apnea, which may affect repair capacity and nervous system sensitivity.
The central idea is that trigeminal neuralgia may not depend on anatomy alone. It may depend on whether the rate of irritation or injury exceeds the rate of biological repair.
What this does not mean
This paper does not claim that sleep apnea causes all trigeminal neuralgia.
It does not claim that vascular pulsatility is the only explanation.
It does not replace established treatments such as medication management, neurological evaluation, imaging, or microvascular decompression when appropriate.
Instead, it proposes a broader framework: in some people, structural nerve vulnerability, mechanical vascular stress, sleep-disordered breathing, oxygenation instability, inflammation, and repair capacity may interact in ways that influence trigeminal nerve sensitivity.
That is why this model is called a hypothesis. It is meant to be tested.
A systems-based way to think about nerve pain
In clinical practice, complex pain conditions often do not fit into a single box. A person may have structural findings, vascular risk factors, poor sleep, inflammation, stress physiology, and nervous system sensitization all interacting at once.
This hypothesis reflects the kind of systems-based thinking we bring to patient care at the Blue Ridge Acupuncture Clinic in Asheville, NC.
Classical Chinese Medicine has long emphasized relationships: how circulation, rest, resilience, emotion, digestion, breath, and the nervous system influence one another. Modern medicine uses different language, but the underlying clinical challenge is often similar: how do we understand complex conditions when multiple systems are interacting at once?
For trigeminal neuralgia and other complex facial pain conditions, the most important first steps remain proper medical evaluation, diagnosis, and imaging when appropriate. But taking a systems approach, we might also ask:
Is the nervous system under repeated stress?
Is sleep disrupted?
Is oxygenation stable at night?
Are vascular or inflammatory factors contributing?
Is the body’s repair capacity being supported?
The Trigeminal Triad hypothesis invites clinicians and researchers to look not only at the nerve itself, but also at the conditions that may determine whether the nerve can recover, stabilize, or remain sensitized.
Article Citation
Whittle JC. The Trigeminal Triad: A Rate-Dependent Model Linking Neurovascular Compression, Vascular Pulsatility, and Sleep-Disordered Breathing in Trigeminal Neuralgia. Medical Hypotheses. 2026. doi: 10.1016/j.mehy.2026.111992
Read the article here: https://doi.org/10.1016/j.mehy.2026.111992
For Patients:
If you are dealing with trigeminal neuralgia or complex facial pain, this article is not a substitute for medical diagnosis or treatment. But it may help explain why a broader systems-based evaluation can matter.
At the Blue Ridge Acupuncture Clinic, we approach chronic pain by looking at the whole person: nervous system regulation, sleep, stress physiology, inflammation, circulation, and the body’s capacity to recover.
To learn more or request an appointment, please contact the Blue Ridge Acupuncture Clinic:
Call or text: (828) 254-4405
Email: info@blueridgeclinic.com
Web: blueridgeclinic.com